Drop the Term “Accessory” Vein Consensus Emerges
It was announced today that members from Inovia Vein participated in an international anterior saphenous vein consensus task force to address the confusion around the term “accessory.” From this a drop the term “accessory” consensus emerged. Edward Boyle, MD and Rachel Drgastin participated as invited members of the task force. This task force was convened by the American Vein and Lymphatic Society (AVLS), in collaboration with the Union International of Phlebology (UIP) and the American Venous Forum (AVF), Their mission was to evaluate the need to evolve the nomenclature internationally of the Anterior Accessory Saphenous Vein (AASV).
Task Force Members
Members included: Mark Meissner, MD, Department of Surgery, University of Washington, Seattle, WA; Alberto Caggiati, MD, Department of Anatomy, University “La Sapienza,” Rome, Italy; Antonios Gasparis, MD , Northwell Health Department of Vascular Surgery, Greenlawn, NY; Nicos Labropoulos, Ph.D., Stony Brook Medicine, Stony Brook, NY; Suat Doganci, MD, Gulhane School of Medicine, Ankara, Turkey; Rachel Drgastin, BS, Oregon Health Sciences University, Portland, Oregon; and Edward M Boyle, MD, Founder and Director of the Inovia Vein Specialty Centers, Bend, Oregon. This group embarked on a mission to review existing anatomical and clinical literature related to the AASV and propose alternative terminology to mitigate confusion that the term “accessory” creates.
The Need to Address the Confusion from the Term Accessory
ASV reflux occurs in nearly 1 in 5 patients presenting for the first time for treatment and is fast becoming the most common cause of recurrence in patients who have had prior varicose vein treatment. To some the use of the word “accessory” implies that the vein is a superficial tributary. This has led to confusion on the best treatment modalities to achieve the optimal long term outcomes. Anatomic and clinical evidence supports its role as a truncal vein, similar to the great and small saphenous veins. This is important because truncal or axial veins have different treatment requirements compared to branch tributary veins in order to optimize long term treatment outcomes. However, the term Accessory is confusing and suggest this is a branch varicosity. This lack of clarity can lead to confusion in coverage policies that ultimately limit access to treatments and impact our patient’s outcomes.
The Consensus Process
The process involved a collaborative effort over several years among medical professionals and researchers. The resulting consensus was endorsed by the major venous specialty societies.
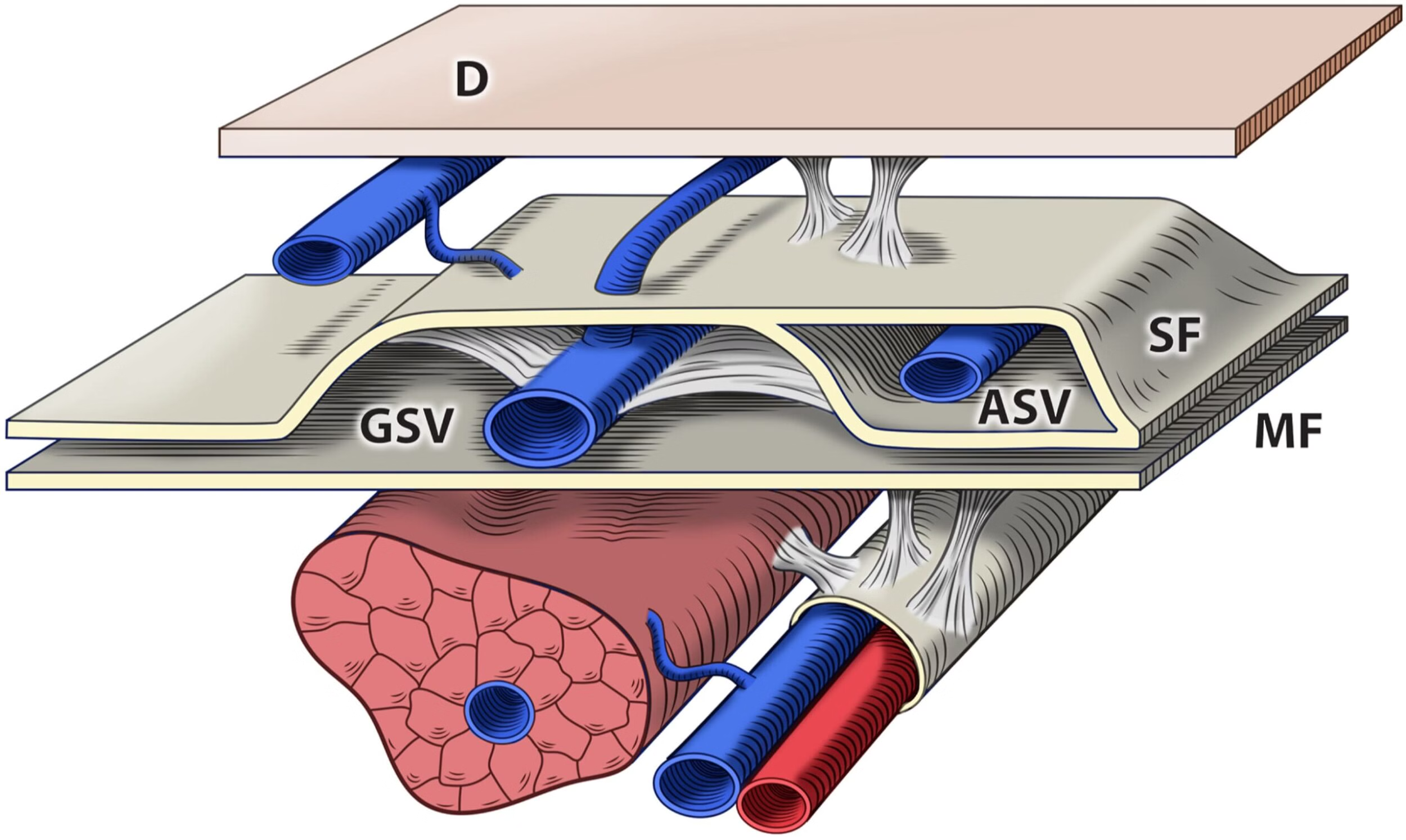
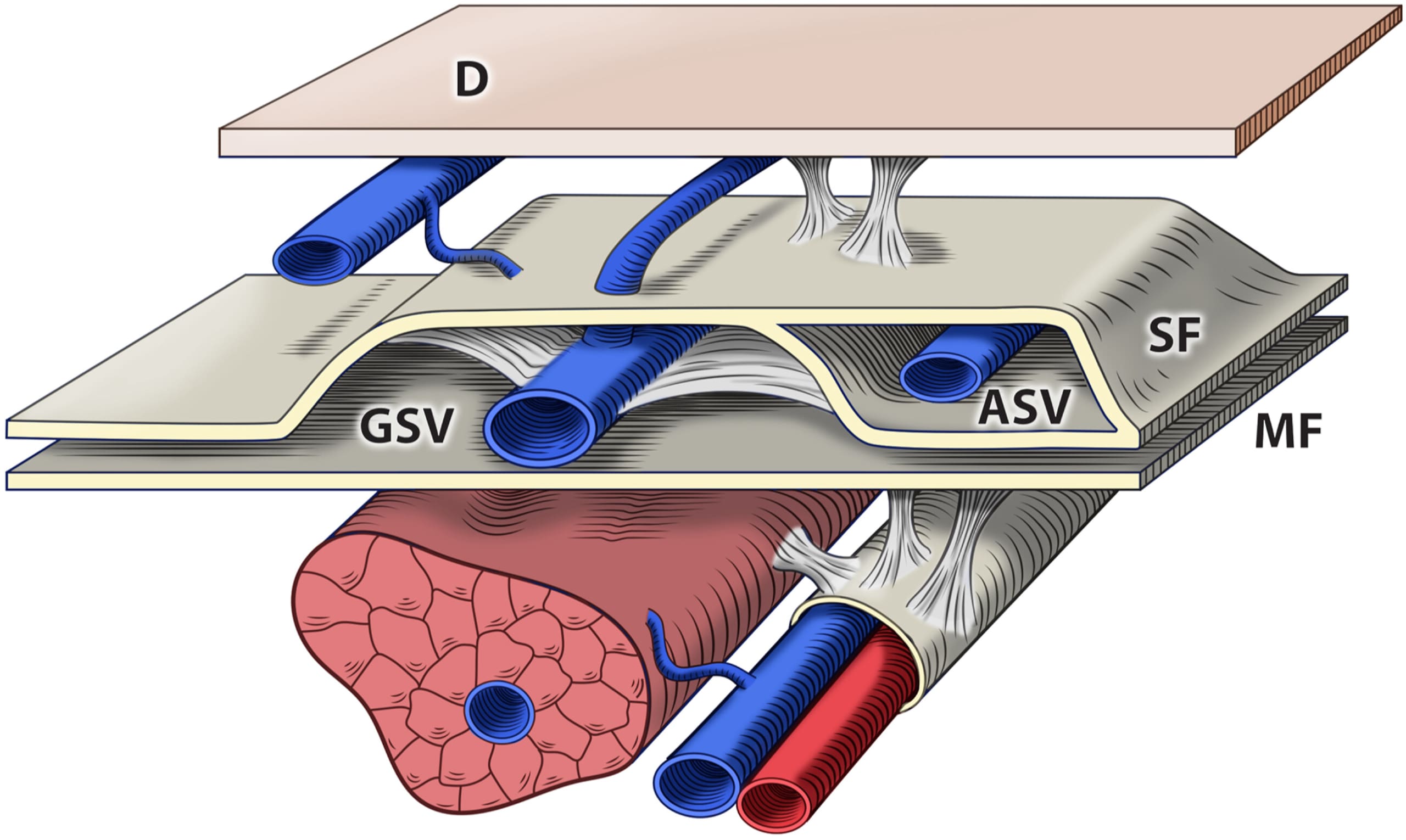
To form this consensus, the group addressed the history of the confusion surrounding the anterior accessory saphenous vein (AASV). This was due to varying definitions based on anatomical dissections and duplex ultrasound findings in the past. It was noted that for many years there was a broad definition of accessory veins that led to ambiguity regarding whether these veins were situated inside or outside the saphenous compartment. In the superficial leg compartment, veins in the their own compartment should be classified as axial or truncal veins, and those outside the fascia as branch varicosities.
In recent years with review of the duplex anatomy improved a refined anatomical nomenclature was established which suggested the need to evolve this term. From this it became clear the ASV is located in its own saphenous compartment lateral to the great saphenous vein (GSV). As such, the group concluded, the ASV is not simply just a branch varicosity off the GSV but is an axial vein in its own right.
The Conclusion: Drop the term “accessory”
From this process a consensus emerged that the term “accessory” should be dropped. Now it is suggested the vein simply referred as the anterior saphenous vein (ASV).
The Significance
Treatment approaches for ASV have the best outcomes when they utilize axial vein treatment strategies like radiofrequency ablation, laser ablation, or other forms of axial vein closure rather than branch varicosity treatment strategies such as phlebectomy or ultrasound guided sclerotherapy.
“The longstanding confusion surrounding the term “anterior accessory saphenous vein” has resulted in misconceptions regarding its anatomy, clinical significance, and treatment implications,” said Dr. Mark Meissner. “The term ‘accessory’ has perpetuated misunderstandings about the true nature of this vein and its clinical relevance,” emphasized Dr. Meissner. “In order to ensure optimal access and outcomes for patients, there was consensus that we revisit and refine the anatomical designation.”
Alberto Caggiati, MD, Professor of Anatomy at the University “La Sapienza,” Rome, Italy, led the review of the anatomical considerations. “The anterior saphenous vein is a truncal vein akin to the great and small saphenous veins and not a branch tributary.” “The anatomic rational is that the ASV has a distinct envelopment in its own fascia in the upper leg.”
“It was imperative to address the tangible impact of terminology confusion on patient care,” said Dr Edward Boyle. “A more accurate designation of its status as a truncal vein is important in selecting the most appropriate axial treatment options. That helps us best offer proven evidenced based treatments that optimize long-term patient outcomes in the management of this common venous condition.”
Links to the Open Access Publications
This collaboration culminated in the simultaneous publication of a series of four manuscripts. They were submitted to Phlebology and the Journal of Vascular Surgery Venous and Lymphatic Disorders for peer review. Endorsement by the sponsoring societies to drop the term “accessory” vein followed. After acceptance the two major vein treatment journals agreed to release all four of them simultaneously in March 2024. These comprehensive publications review in depth the anatomy, provide a systemic review of the literature, an evaluation of current payer policies, and explore treatment considerations pertinent to the anterior saphenous vein.
Phlebology: The Journal of Venous Disease